Bridging the Semantic Gap: Natural Language Processing and Symptom Network Analysis
[The Clinical-Narrative Gap and Ontological Redefinition ]
A fundamental challenge in contemporary medicine is the discordance between standardized clinical terminology and the lived experience of patients. Traditional medical frameworks define and assess symptoms using rigid, physician-constructed questionnaires and diagnostic criteria, which often reduce complex human experiences to binary or scalar variables. However, patients rarely communicate their suffering using this formal vocabulary; instead, they employ rich, nuanced, and metaphorical language, particularly within the uncontrolled environments of social media and online health forums. This research addresses this critical semantic and ontological gap by redefining patient-generated text not as mere subjective anecdote, but as a vast, unstructured repository of high-dimensional, structured clinical information. We propose a paradigmatic shift that treats patient narratives as organized semantic systems susceptible to rigorous quantitative analysis. By leveraging large-scale data science techniques, we aim to decode how patients cognitively organize and communicate their symptom experiences, thereby transitioning from a purely clinician-centric model of symptom definition toward a semantic model rooted in the authentic voice of the patient.
[NLP, Discrete Mathematics, and Motif Identification]
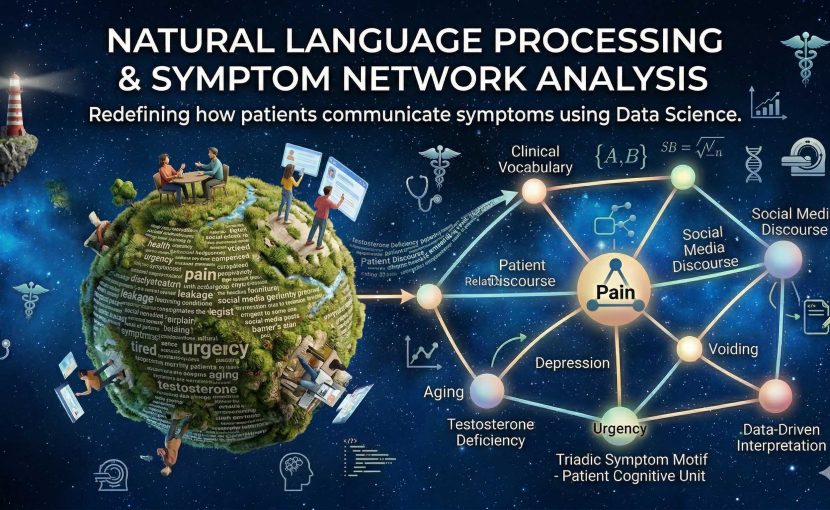
The methodological core of this research involves a multi-staged computational pipeline integrating Natural Language Processing (NLP), discrete mathematics (specifically graph theory and topology), and unsupervised machine learning. We analyze massive datasets comprising hundreds of thousands of words from patient-generated online discourse. NLP algorithms are first employed for semantic extraction, transforming unstructured text into structured symptom vocabularies. These extracted terms are then modeled as nodes within a discrete relational network, where edges represent probabilistic co-occurrence and semantic proximity. A crucial innovation is the application of discrete mathematical constraints to identify stable, higher-order topological patterns within these semantic networks. We consistently observe that patient discourse does not form random associations; rather, it organizes into stable structural motifs. Specifically, we have identified unique triadic symptom motifs—such as the triangulated relationship between pain, urgency, and voiding—which serve as the minimal, robust units of cognitive symptom organization. Unsupervised learning further allows us to phenotype these structures, revealing previously unrecognized symptom clusters and central hubs that function as semantic bridges between disparate medical domains.
[Integrated Vision and Clinical Transformation ]
The integration of NLP and symptom network analysis provides a powerful, quantitative framework for bridging the divide between standardized clinical terminology and patient experience. This approach demonstrates that traditional vocabulary often underrepresents key symptom relationships that are central to patient suffering. Furthermore, it reveals that patient narratives contain reproducible structural information far beyond the sum of individual terms. Our unifying framework transforms these narratives from qualitative descriptions into precise, multidimensional data structures that reflect the true systemic nature of the patient’s condition. The ultimate goal of this research is to operationalize this Symptom Structure Science within clinical practice. By converting the rich texture of patient discourse into data-driven, mathematically precise models, we can enhance patient-physician communication, improve the accuracy and nuance of symptom assessment tools, and develop novel, patient-centered diagnostic phenotypes. This research establishes a critical interface between data science and clinical medicine, enabling a shift toward a truly personalized and data-driven approach where clinical interpretation is informed and refined by the authentic structure of patient language.