Journal of the Laser and Health Academy
Vol. 2021, No.1; www.laserandhealth.com
CASE REPORT: Effects of transrectal non-ablative prostate
Erbium:YAG laser treatment on a hemiplegic patient with
erectile dysfunction and urge incontinence
Nobuo Okui1,2, Machiko Okui2, Zdenko Vizintin3, Matjaz Lukac3
1 Kanagawa Dental University, Yokosuka, Kanagawa, Japan 2 Uro-Gyn.Net Health Care Cooperation, Dr Okuis’ Urogynecology and Urology Clinic, Yokosuka, Kanagawa, Japan 3 Fotona, d.o.o., Ljubljana, Slovenia, EU
ABSTRACT
Introduction: Brain stroke survivors often experience erectile dysfunction (ED). Pharmacotherapy with phosphodiesterase-5 (PDE5) inhibitors is one of the first-line therapies for ED, but it is contraindicated in patients taking nitrites. The quality of life is markedly lower in patients whose condition is also complicated by urge incontinence.
We propose non-ablative erbium: yttrium aluminum garnet (YAG) laser treatment (EL) as a therapeutic approach for these refractory diseases. The
efficacy of transvaginal non-ablative EL irradiation in the treatment of women with sexual dysfunction and urge incontinence without causing adverse effects has been reported.
Aim: Our aim is to report the case of a 62-year-old hemiplegic man whose ED and urge incontinence improved after transrectal non-ablative prostate EL (TR-PEL).
Methods: Ten-minute TR-PEL was performed monthly for 9 months and the effect on ED and urge incontinence was evaluated.
Conclusions: ED and urge incontinence both improved dramatically without side effects. TR-PEL is a promising new treatment procedure.
This is an initial report describing the effective use of non-ablative EL in the treatment of a male patient.
I. INTRODUCTION
Erectile dysfunction (ED) [1] is the consistent or recurrent inability to attain and/or maintain penile erection sufficient for sexual satisfaction. In particular, 48.3% of stroke survivors experience ED. [2]
Phosphodiesterase-5 inhibitors (PDE5is) are the firstline therapy for ED but PDE5i treatment is contraindicated in patients using nitrites because additive vasodilatory effects may cause systemic vasodilation and marked hypotension. [3]
Angina and arrhythmia are some of the causes of cerebral stroke, and many patients with these conditions take nitrites. Furthermore, the quality of life markedly decreases in patients with stroke complicated by urge incontinence. [4] At present, no treatment exists for such refractory cases.
The present case report focuses on non-ablative vaginal erbium: yttrium aluminum garnet (YAG) laser treatment (VEL), [5-7] which has been reported to be effective for treating sexual dysfunction [5], stress urinary incontinence (SUI) [6] and overactive bladder (OAB) [7] in women without adverse effects.
Improvement of the vaginal mucosa improves the sexual function. Transvaginal application extends the effects of laser treatment beyond the surface to the bladder and urethra and has been confirmed to improve SUI. A procedure of transrectal irradiation of the periprostatic area—transrectal non-ablative prostate erbium: YAG laser treatment (TR-PEL)— may be a promising new treatment for improving urge incontinence or ED.
This is an important report that describes the successful treatment of ED and urge incontinence in a patient with refractory symptoms.
II. CASE REPORT
The patient was a 62-year-old man who developed angina at 50 years of age and had a cerebral infarct at age 60 years that left him hemiplegic on the left side. He developed ED and urge incontinence at the same time, which has persisted to date. At the initial examination, he was assessed as Brunnstrom stage 4 [8] with decreased spasticity: stage 4 in the arm, hand, and leg on the left side. Transrectal ultrasound revealed that the size of the prostate was normal (35 × 20 × 25 mm, 9.16cc). The New York Heart Association (NYHA) class was classified as 2 and movement of 6 metabolic
equivalents (METs) was possible. He had quit smoking at 50 years of age and was taking hypotensive drugs (angiotensin-converting enzyme inhibitors [ACE]). He was continuing to take anticoagulant therapy with warfarin potassium and aspirin. He was also taking nitrites. Drug-induced ED, depression, sleep apnea, diabetes, kidney and liver dysfunction were excluded in the department of internal medicine.
According to the Princeton Consensus Panel, [3] a NYHA class 2 patient can be treated to improve sexual dysfunction, but PDE5is are contraindicated in patients possibly taking nitrites and there are no alternative treatments; thus, we determined that TR-PEL with local anesthesia could be indicated for this patient. The lithotomy position was used during the treatment.
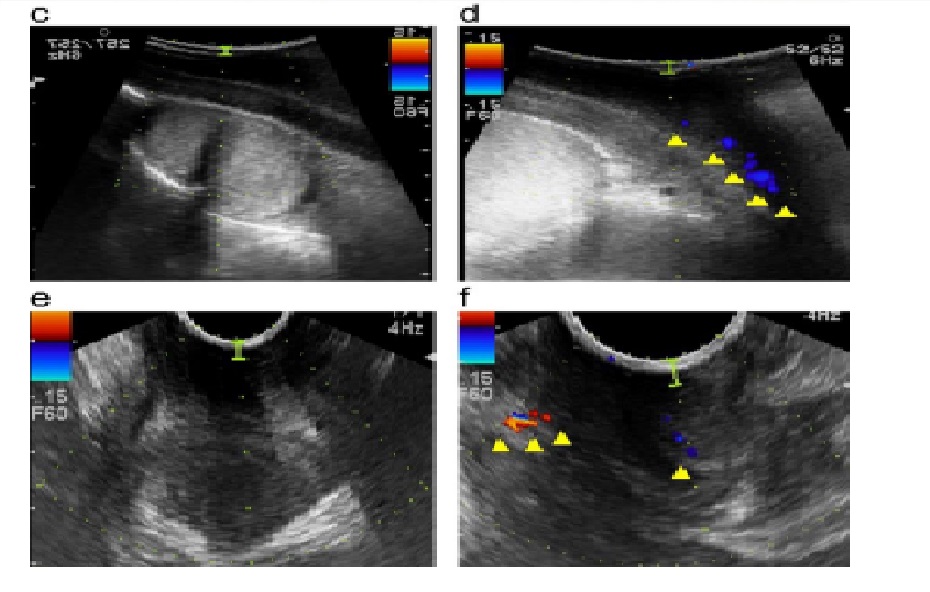
First, a preoperative transrectal diagnostic ultrasound (DUS) test (F37 and EUP-U531 HITACHI- ALOKA, Tokyo, Japan) was used to observe periprostatic and cavernous blood flow. Next, Xylocaine pump spray 8% (Aspen Japan, Tokyo, Japan) was applied to the anus for local anesthesia for TR-PEL and an anus-sized handpiece, SmoothTouch LA Adapter connected to a FotonaSmooth™XS (Fotona d.o.o.) laser was inserted and positioned under the prostate. Approximately 5 cm of the periprostatic area was irradiated for 10 min using a non-ablative 2940 nm Er:YAG laser on long pulse (Smooth) mode, with following settings: 3.00 J/cm2,
2.0 Hz, 7 mm. [5] Since there was no report of a nonablative laser treatment applied to the rectal mucosa, we thought that an endoscope was needed.
Proctoscopy immediately after the procedure confirmed no inflammation of the rectal mucosa. TRPEL was performed monthly for 9 months without
any preparation. The patient was assessed at baseline and during 9 months of treatment using the International Index of Erectile Function (IIEF), [2]
the 5-item version of IIEF (IIEF-5), [9] the overactive bladder symptoms score (OABSS), [6] the International Consultation of Incontinence Questionnaire – Short Form (ICIQ-SF), [5] the International Prostate Symptom Score (I-PSS), [4] the amount of daily incontinence confirmed by a bladder diary, the frequency of nocturia, a 1-hour pad test, [6] the DUS of the prostate and penis, and photos of the patient’s morning erection. Measurement of prostatespecific antigen (PSA) (CLIA method, BML Tokyo Japan), serum total testosterone (TT) (CLIA method, BMI), BUN, and Cr blood tests (UV method, BML) were performed at 9:00 a.m. An intracavernous injection of prostaglandin E1 test was unfeasible due
to major bleeding caused by the procedure. We used urodynamic, pressure flow and uroflowmetries (EDAP TMS, Lyon, France). The urodynamic and
pressure flow evaluation could not be measured accurately due to urethral bleeding from the catheter type instrument. As this report is the 1st case of TRPEL, follow-up for adverse events included monthly visits for blood tests and genital and rectal examinations.



この記事へのコメントはありません。