Testosterone, Frailty, and Systemic Aging: A Decisive Shift Toward System-Level Biomarker Networks
[Problem Redefinition and Ontological Mandate]
Conventional medical ontology predominantly conceptualizes biological markers, such as testosterone, as solitary entities. Treatment decisions are often made based on local biological thresholds, treating similar biological levels as functionally identical across individuals. However, this fragmented approach is insufficient for characterizing complex, systemic biological states like frailty and aging. Clinical context matters fundamentally; similar biological levels can reflect profoundly different underlying biological states depending on their interaction with dynamic and non-linear variables, including systemic inflammation, metabolic shifts, and declining organ function. The present research addresses this limitation by proposing a definitive transformation of the medical ontology: the shift from viewing testosterone as an isolated variable to conceptualizing it as an organized, high-dimensional, and structured relational system. Utilizing an immense real-world clinical dataset accumulated from high-volume, longitudinally followed surgical and medical practices, we apply high-order network science, discrete mathematics (including graph theory and topology), and data science techniques like unsupervised clustering. This integration enables us to model the intricate, discrete relational structures linking hormonal variables, inflammatory markers, renal and metabolic parameters, and diverse functional outcomes, facilitating a nuanced, systemic-level interpretation of physiological context.
[Unsupervised Clustering and Network Centrality ]
The methodological cornerstone of this approach is a rigorous, quantitative transformation of multivariate data into structured, actionable networks. A key innovation of this work is the dynamic identification of higher-order topological patterns within these discrete relational models. Unsupervised machine learning, in the form of unsupervised clustering, reveals distinct latent patient profiles characterized by non-linear combinations of biomarker variables. Our analysis has identified a striking high-risk aging profile, defined as a discrete relational motif where low testosterone coexists with systemic inflammation and impaired renal function. Importantly, this high-risk pattern is a coordinated biological state, not a simple hormonal abnormality. Network analysis further demonstrates that the mathematical importance (centrality) and relationship of testosterone are not fixed across individuals, but dynamically vary depending on the surrounding physiological context. Crucially, this research extends beyond male populations. Clinical studies in women show that testosterone is strongly associated with functional aging processes and urinary incontinence, particularly when integrated into a structured, high-dimensional network model. By treating these high-order network structures as dynamic mathematical objects, we can predict systemic response patterns and functional decline with unparalleled precision, reducing the trial-and-error approach common in traditional biomarker interpretation.
[Redefining Outcomes and Bridging Ontological Gaps]
This paradigmatic shift necessitates a comprehensive redefinition of clinical outcomes. Traditional medicine often measures success by single endpoints, such as “is the biological marker corrected?” or “is the primary symptom eliminated?” In real-world clinical practice, however, success is multidimensional. Our framework interprets functional decline as a multi-domain structured patient experience, integrating biological data (hormone levels, biological markers) with qualitative metrics (quality of life, pain reduction, sexual function, return to daily activity). By treating this multi-domain structure as an interconnected relational network, we can quantitatively model the impact of therapeutic interventions across diverse patient-centered experience domains. The methodology transforms subjective patient language and experience into precise, structured clinical data points within this structured biomarker network. This bridge-building between formalized quantitative metrics and lived qualitative experience is central to our mission. It allows us to formalize and systematize personalized clinical strategies, providing a precise, data-driven foundation for precision medicine tailored to the structural reorganization of each individual patient’s condition, moving beyond simple reductive choices toward a systemic-level optimization.
[A New Model of Medicine: The Systemic Translator ]
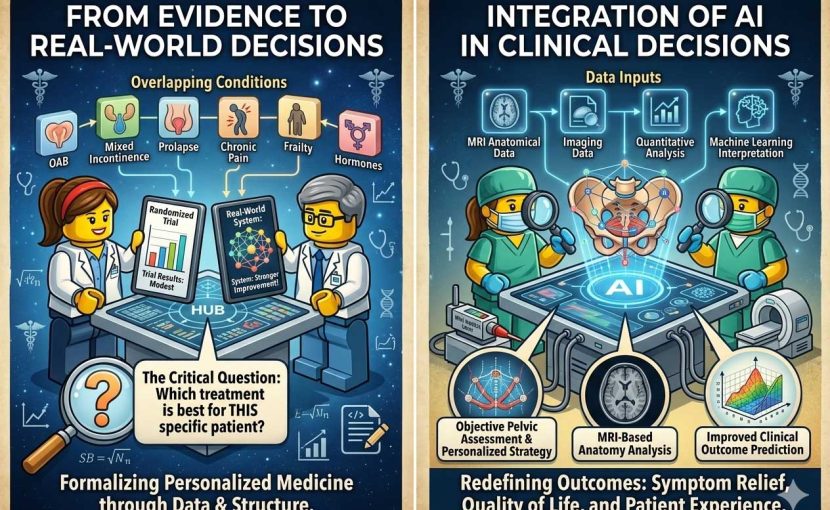
The ultimate vision of this research is not simply to corrective biological levels, but to operationalize a truly new clinical paradigm: Symptom Structure Science. The entire conceptual vision, visually illustrated as a bridge between a detailed narrative world and a high-order mathematical decision network, conveys this decisive shift. On the left side of this conceptual vision, traditional biological elements analyze organs independently. On the right, digital interfaces and artificial intelligence (AI) precise represent the integration of real-world patient narratives, quantitative analysis, and mathematical modeling, providing previously unobserved structured clinical insights. This framework serves as a sophisticated translator, transforming reductionist biological signals into systemic, relational models that reflect the true complexity of human aging. By unifying high-volume, longitudinally followed surgical practice with diverse clinical data, advanced mathematics, and patient-reported outcomes, Symptom Structure Science establishes a powerful new interface between quantitative precision and qualitative human suffering. This unifying framework facilitates a definitive paradigmatic transformation, enabling personalized and truly patient-centered medicine by guiding clinical decision-making based on the authentic topological structure of a patient’s aging condition. This entire ecosystem forms a cohesive translational cycle: clinical practice → data collection → analysis → new treatment → clinical application, ensuring research and clinical practice are parts of a single evolving system.